Articles
Jul 8, 2026
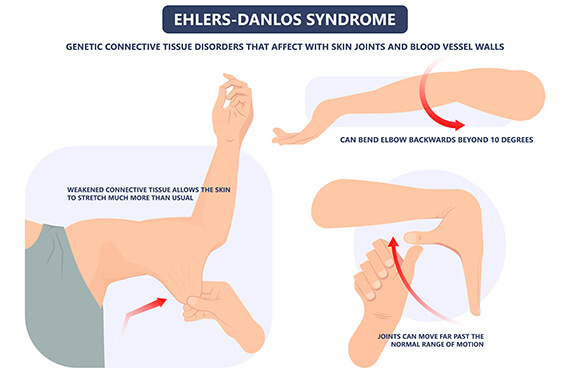
What is Ehlers-Danlos syndrome (EDS)? Symptoms, causes and rehabilitation
It’s more than hypermobility. That’s what any rehabilitation specialist will tell you if you’ve been diagnosed with the connective tissue disorder Ehlers-Danlos syndrome (EDS).

Connective tissue is everywhere — it’s in our heart, lungs, eyes, skin, cartilage, bones, tendons, ligaments and more. It literally holds the body together, creating a framework that supports, protects and integrates all other tissues.
As an extensive, sometimes disabling condition, EDS can impact multiple systems. Let’s learn more about EDS and how it can affect the whole body while remaining one of the most misunderstood diagnoses.
Difficult to diagnose
With symptoms that vary widely and overlap other conditions, EDS is complex and difficult to diagnose. EDS is often confused with chronic fatigue syndromes, autoimmune diseases and hypermobility spectrum disorder (HDS).
HDS (also a connective tissue disorder) has many of the same symptoms as EDS, but based on severity or prevalence, those symptoms don’t rise to meet the criteria of EDS or have a multi-system impact.
There is currently no single test that says, yes, you have EDS. Researchers are working to find a clear path to diagnosis.
For now, an official diagnosis is generally found through a primary care provider who assesses joint hypermobility and skin stretchiness. Genetic blood or saliva tests are used to confirm rare subtypes, but the most common form, hypermobile (hEDS), requires clinical criteria to diagnose and has no genetic markers.
The WHO of EDS
EDS primarily impacts young females, with 70% to 80% of diagnosed patients being biologically female. Why females? Research suggests that fluctuations in estrogen may affect connective tissue instability and symptom severity, often leading to worsening symptoms around puberty.
But biological males are not out of the equation. Men can and do endure EDS and related disorders. And, even though EDS and HDS are underdiagnosed, they can be just as severe and debilitating in men as they are in women.

Symptoms typically emerge in childhood and adolescence, with diagnosis frequently peaking in teenagers for women and slightly earlier (ages 5 to 9) for men. The average age of those heavily impacted and surveyed sits around 35 to 37 years old.
For those seeking rehabilitative care, many present with joint instability, lacking the robust ligaments needed to hold their bones together. Muscles also don’t contract as efficiently or respond to the nervous system as effectively as those without EDS. Patients can struggle to locate and activate muscle groups when they want to.
The most common complaint is joint pain, but the symptoms cross the whole spectrum. People can have milder forms where they don’t have a lot of other body-system issues but may feel a little bit more flexible than what is normal. On the other end, EDS can be disabling where individuals have trouble getting out of bed and one simple daily activity may take all the energy they have for the day.
EDS symptoms
Symptoms of EDS can often mimic others or easily be overlooked at first. EDS symptoms include:
- Joint issues: Loose joints, clicking joints, recurrent dislocations and flat feet
- Skin issues: Extremely soft, velvety skin that easily stretches and is fragile, with slow wound healing and abnormal, wide scars
- Pain and fatigue: Widespread musculoskeletal aching, persistent and extreme tiredness and muscle weakness
- Gastrointestinal: Frequent bloating, heartburn, constipation, gastroparesis and irritable bowel syndrome (IBS)
- Cardiovascular: Dizziness and rapid heart rate upon standing, poor circulation and potential heart valve issues
- Neurological and cognitive: Brain fog, trouble concentrating and chronic headaches
- Pelvic and bladder: Loss of bladder control (incontinence) and organ prolapse
Navigating life with EDS through rehabilitation
Rehabilitation, physical and occupational therapy, can be the key to coaxing the body to cooperate for people living with EDS.
There are benefits to starting rehabilitation for EDS at a young age. Therapists can focus on preventive physical therapy before the body actually starts hurting.
Hypermobile kids tend to treat their flexibility as a “party trick” or something they show off, stretching their bodies in ways that may not hurt at the moment. The more young patients can be taught to protect their joints and what movements not to do, the better.
Hyperfocused on stabilizing joints, managing chronic pain and improving daily function through muscle strengthening and posture correction, therapy experts educate how normal muscle and joint function works and how the person with EDS can identify their own muscle and joint response for productive movement.
Movement looks different for someone with EDS. Strengthening deep and superficial muscles around the joints is a primary defense. Unlike regular strengthening, therapists work instead on repetition and quality of movement with lower loads like using your own body weight, resistance bands or minimal weights to increase endurance and motor control.

Rehabilitation works also to find balance and coordination by helping individuals know where their limbs are in space and how using these vital controls in proper positions can prevent accidental injury.
Therapists also consider how the neuromuscular system is working with the mechanics of an EDS body. They work to retrain the nervous system to fire muscles to move safely and efficiently during daily activities without overextending joints.
Manual therapy, or gentle hands-on techniques applied by an expert clinician, can reduce muscle spasms, relieve trigger points and alleviate tension that can build up in muscles as they compensate for loose joints. Physical therapists focus on:
- Joint, muscle and nerve mobilization
- Joint mobilization and muscle energy techniques
- Myofascial release/soft tissue mobilization
- Trigger point therapy
- Strain counterstrain or positional release therapy
Tools in the EDS rehabilitation toolbox
Some valuable tools therapists can use to enhance their work with EDS patients include specialized techniques or resources to make life more manageable.*
Aquatic therapy can provide a safe exercising environment, providing buoyancy, which reduces joint stress and allows for productive movement and resistance during periods of severe pain or flare-ups.
Pelvic floor therapy is used to treat associated chronic pain, organ prolapse (when organs drop or bulge because of weak muscles) and bladder and bowel dysfunction.
Orthotic and bracing support can be crucial for temporary use as patients work under the guidance of their therapist to reinforce joint alignment while muscles are being developed. This could include braces, kinesiology tape and custom shoe orthotics.
Therapists may use pain management techniques, including hot or cold therapy, transcutaneous electrical nerve stimulation (TENS) and dry needling to manage pain.
EDS patients often have fingers that bend backward easily and joints (like at the base of the thumb or knuckles) frequently slip out of place. Occupational therapists who are certified in hand therapy can provide gentle strengthening and joint protection techniques as well as different splints, braces and adaptive tools.

Prevention of and recovery from injury looks different
For people with EDS, the degree of mobility and flexibility they experience feels normal to them. They don’t necessarily realize they’re doing movement incorrectly, they’re just moving the way they’ve always moved. Their bodies get very good at getting the job done, not usually in the correct or safest way.
This abnormal movement can often lead to worsening joint instability and it is common for individuals to experience dislocations (when a joint comes completely out of the socket) or subluxations (partially out of the socket) and there’s always a risk that something gets pinched or torn during the process.
Therapists work on injury repair with an EDS patient in a different way on something like a shoulder tear. The methods of building back strength will look different than with a standard orthopedic patient, taking into consideration the special physical circumstances of EDS.
Making adjustments to how the body moves and is cared for under the guidance of a skilled therapist can be life changing for someone living with EDS.
When flare-ups occur, which may look like everything hurting just a bit more than normal, it is especially important for the EDS individual to modify their activity and working with a therapist can help calm the nervous system. When the nervous system is fired up during a flare, the brain can perceive what they are feeling as more intense and they can be hypersensitive to pain.

Reexamining types of EDS
There are currently 13 different types of EDS. Many of them can be addressed with rehabilitation to bring better and more managed movement and mobility to life.
- Hypermobile EDS (hEDS): The most common type. It causes highly unstable/loose joints, recurrent dislocations and chronic pain, but lacks a known genetic cause.
- Classical EDS (cEDS): Highly stretchy, velvety skin that bruises easily, along with widened, atrophic scars after injuries.
- Vascular EDS (vEDS): The most severe type. It causes fragile blood vessels and organs that are prone to spontaneous rupture.
- Cardiac-valvular EDS (cvEDS): Affects the heart valves, causing severe, progressive cardiac issues alongside joint and skin symptoms
- Arthrochalasia EDS (aEDS): Characterized by severe, generalized joint hypermobility and hip dislocations present at birth.
- Dermatosparaxis EDS (dEDS): Features exceptionally fragile, sagging skin that tears easily, severe bruising and hernias.
- Kyphoscoliotic EDS (kEDS): Causes severe curvature of the spine (kyphoscoliosis) that appears in early infancy, as well as weak muscle tone.
- Brittle cornea syndrome (BCS): Causes severe thinning of the corneas, which can lead to rupture, along with blue whites of the eyes.
- Classical-like EDS (clEDS): Similar to cEDS, featuring velvety skin and joint hypermobility, but without the scarring.
- Musculocontractural EDS (mcEDS): Causes fixed joints at birth, distinct facial features and severe skin fragility.
- Myopathic EDS (mEDS): Present at birth with congenital muscle weakness and contractures in large joints, along with hypermobility in smaller joints.
- Periodontal EDS (pEDS): Results in early-onset, severe inflammation of the gums (periodontitis) causing premature tooth loss.
- Spondylodysplastic EDS (spEDS): Causes short stature, muscle weakness and skeletal abnormalities.
At the end of 2026 and beginning of 2027, the Ehlers-Danlos Society is releasing a major update to global EDS and HSD diagnostic criteria.
New international research and clinical findings have prompted the International Consortium to reevaluate disease definitions to improve diagnostic accuracy. The upcoming updates will refine hypermobility measurements, improving how joint mobility is evaluated to separate true hypermobility from general flexibility. The changes will also address misdiagnosis, giving patients and healthcare providers more power in earlier diagnosis and treatment.
Based on the new recommendations, our therapists will adjust care plans and treatments to answer what research shows as the latest known factors of EDS.
Evolving condition, expert care
There is no cure for EDS.
Building a relationship with rehabilitation as part of living with EDS maximizes overall function. With expert therapist assistance, EDS individuals can find ways to do as much as is physically safe to do and walk away with the tools and resources they need to be empowered to take care of themselves.

Physical therapists, and especially physical therapists with EDS-specific training, can make the unstable feel stable and give anyone living with EDS the control they seek to succeed in daily life and for the long term.
Rehabilitation provides EDS patients with control — control over pain, movement and life.
Clinical contribution to this blog provided by Physical Therapist Michaela Clemens.
*Services vary by location.